

Semaglutide has become one of the most talked-about medications in weight management. Known under brand names Wegovy® and Ozempic®, it has shown clinically significant results in large-scale trials — but it is also a prescription medication with a structured dosing protocol, real contraindications, and side effects that are frequently misunderstood.
This guide walks you through exactly how semaglutide works, what the evidence says, how dosing progresses, and what you need to discuss with your doctor before starting.
Pharmacist’s Perspective — Faryal Faisal, PharmD
Before anything else, I want to address the most common mistake I see with semaglutide: patients rushing the dose escalation schedule to reach results faster.
The titration timeline — starting at 0.25 mg and increasing gradually over weeks — is not a suggestion. It exists because your GLP-1 receptors need time to adjust to the medication. Patients who skip ahead or increase too quickly almost always experience severe nausea and vomiting that leads them to abandon the medication entirely. Patience with the escalation schedule is not optional — it is clinically the difference between completing the treatment and quitting it.
Second: always tell your prescribing doctor your complete medication list before starting semaglutide — not just the medications you think are relevant. Semaglutide slows gastric emptying, which directly affects how quickly other oral medications are absorbed. This matters especially for oral contraceptives, thyroid medications, and blood thinners. A pharmacist or physician needs to review your full regimen before you begin.
— Faryal Faisal, PharmD, Start Being Healthy
What Is Semaglutide?
Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist — a synthetic version of a hormone your gut naturally releases after eating. It was originally developed for type 2 diabetes management, where it helps regulate blood sugar by stimulating insulin release and suppressing glucagon. Its effect on weight loss was identified during diabetes trials and subsequently studied in dedicated obesity programmes.
In 2021, the FDA approved semaglutide 2.4 mg (Wegovy®) specifically for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related condition such as hypertension, type 2 diabetes, or high cholesterol.
Ozempic® (semaglutide 0.5–2 mg) remains FDA-approved for type 2 diabetes, though it is frequently prescribed off-label for weight loss.
How Semaglutide Works for Weight Loss
Semaglutide acts on GLP-1 receptors in the brain, pancreas, and gastrointestinal tract simultaneously:
Appetite suppression — It activates GLP-1 receptors in the hypothalamus, the brain region responsible for hunger regulation, reducing appetite and food-seeking behaviour.
Delayed gastric emptying — It slows how quickly food leaves the stomach, which extends the feeling of fullness after meals and reduces caloric intake naturally.
Insulin regulation — It stimulates glucose-dependent insulin secretion, meaning insulin is released in response to blood sugar elevation — not independently, which lowers the risk of hypoglycaemia in non-diabetic patients.
Glucagon suppression — It reduces glucagon release from the pancreas, decreasing the liver’s glucose output and contributing to better blood sugar stability.
The net effect is a significant reduction in caloric intake without requiring conscious restriction at every meal — which is why clinical trial weight loss outcomes with semaglutide are substantially larger than those achieved by diet alone.
What the Clinical Evidence Shows
The STEP (Semaglutide Treatment Effect in People with obesity) trial programme is the most comprehensive clinical evaluation of semaglutide for weight management to date.
STEP 1 Trial (2021) — The landmark trial enrolled 1,961 adults with obesity or overweight (without diabetes) and randomised them to semaglutide 2.4 mg weekly or placebo for 68 weeks, alongside lifestyle intervention. The semaglutide group achieved a mean body weight reduction of 14.9%, compared to 2.4% in the placebo group. Notably, 86.4% of semaglutide participants achieved at least 5% weight loss, and 50.5% achieved 15% or more — outcomes not previously seen with any approved anti-obesity pharmacotherapy.
(Wilding et al., NEJM, 2021 — PubMed: 33567185)
STEP 2 Trial (2021) — In patients with both obesity and type 2 diabetes, semaglutide 2.4 mg produced mean weight loss of 9.6% versus 3.4% with placebo at 68 weeks. The lower absolute weight loss compared to STEP 1 reflects the physiological challenges of weight management in the context of insulin resistance and diabetes medications.
(Davies et al., Lancet, 2021 — PubMed: 33667417)
STEP 4 Trial (2021) — Patients who achieved weight loss on semaglutide and then switched to placebo regained approximately two-thirds of lost weight over 48 weeks, while those who continued semaglutide maintained their loss. This confirms that semaglutide is a long-term treatment, not a short-term intervention.
(Rubino et al., JAMA, 2021 — PubMed: 33755728)
STEP 5 Trial (2022) — At 104 weeks (two years), semaglutide produced mean weight loss of 15.2% versus 2.6% with placebo, demonstrating sustained long-term efficacy.
(Garvey et al., Nature Medicine, 2022 — PubMed: 35668354)
Semaglutide Dosage Chart — Wegovy® (Weight Management)
The following dosage escalation schedule is the FDA-approved protocol for Wegovy® (semaglutide 2.4 mg) for chronic weight management.
| Week | Dose | Frequency | Route |
|---|---|---|---|
| 1–4 | 0.25 mg | Once weekly | Subcutaneous injection |
| 5–8 | 0.5 mg | Once weekly | Subcutaneous injection |
| 9–12 | 1.0 mg | Once weekly | Subcutaneous injection |
| 13–16 | 1.7 mg | Once weekly | Subcutaneous injection |
| 17+ | 2.4 mg | Once weekly (maintenance) | Subcutaneous injection |
Important: The chart above reflects the approved Wegovy® escalation schedule. The Ozempic® dosing schedule differs and is designed for diabetes management — do not use Ozempic dosing tables to guide Wegovy® use or vice versa. Always follow the schedule prescribed by your physician.
Initial Phase (Weeks 1–4): 0.25 mg
The starting dose is 0.25 mg weekly for the first four weeks. This dose is sub-therapeutic — meaning it will not produce measurable weight loss — and exists solely to allow your body to adapt to the medication and minimise gastrointestinal side effects. Do not increase early if you feel “nothing is happening.” The dose escalation must proceed on schedule.
Titration Phase (Weeks 5–16)
The dose increases every four weeks. Each step builds tolerance and gradually brings the medication toward its therapeutic range. Most patients experience their first noticeable reduction in appetite during this phase, typically around weeks 8–12. Nausea, if it occurs, is usually most pronounced immediately after each dose increase and typically subsides within 5–7 days.
Maintenance Phase (Week 17+): 2.4 mg
The 2.4 mg weekly dose is the established maintenance dose for sustained weight management. Some patients who cannot tolerate 2.4 mg may be maintained at 1.7 mg — this should be discussed with your prescribing physician rather than decided independently.
How to Administer Semaglutide
Semaglutide is administered as a subcutaneous injection — under the skin, not into a vein or muscle.
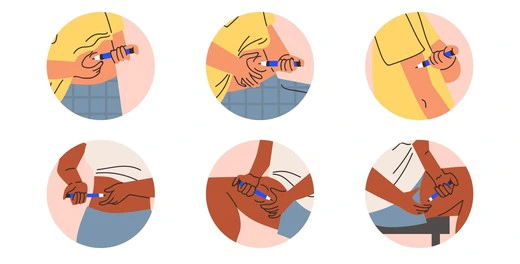
Injection sites: Abdomen (at least 2 inches from the navel), outer thigh, or upper arm. Rotate sites with each injection to prevent tissue hardening or lipodystrophy.
Timing: Inject on the same day each week, with or without food, at any time of day. Consistency in the day of the week matters more than the time of day.
Storage: Unopened pens should be refrigerated (2–8°C / 36–46°F). After first use, Wegovy® pens can be stored at room temperature (up to 30°C / 86°F) for up to 28 days. Never freeze.
Missed dose: If you miss a dose and it has been fewer than 5 days since your scheduled injection, take it as soon as you remember. If more than 5 days have passed, skip the missed dose and resume your regular weekly schedule. Never double dose.
Appearance: Before injecting, check that the solution is clear and colourless. Do not use if it is cloudy, discoloured, or contains particles.
Contraindications — Who Should NOT Take Semaglutide
Semaglutide is contraindicated in the following groups and should not be prescribed to them under any circumstances:
- Personal or family history of medullary thyroid carcinoma (MTC): Semaglutide carries an FDA black box warning for thyroid C-cell tumours based on rodent studies. While large human trials have not confirmed this risk in humans, the precautionary contraindication remains in place for those with MTC history.
- Multiple Endocrine Neoplasia syndrome type 2 (MEN2): Same black box warning applies.
- Pregnancy: GLP-1 receptor agonists should be discontinued at least 2 months before a planned pregnancy. There is insufficient safety data in human pregnancy.
- Severe gastrointestinal disease: Including gastroparesis, as semaglutide further slows gastric emptying and can worsen symptoms significantly.
- Personal or family history of pancreatitis: Semaglutide has been associated with pancreatitis in post-marketing surveillance. Patients with a prior pancreatitis history should discuss this risk explicitly with their physician.
- Type 1 diabetes: Semaglutide is not approved for type 1 diabetes management and carries a risk of diabetic ketoacidosis in this population.
Side Effects
Common (affect >10% of patients)
- Nausea — most common, especially during dose escalation
- Vomiting
- Diarrhoea
- Constipation
- Abdominal discomfort
Most gastrointestinal side effects are dose-dependent and transient — they typically peak immediately after each dose increase and subside within a week. Eating smaller, lower-fat meals and avoiding lying down after eating can significantly reduce nausea severity.
Serious (less common, require medical attention)
- Pancreatitis — Discontinue immediately if persistent severe abdominal pain occurs, particularly if it radiates to the back
- Gallbladder disease — Rapid weight loss from any cause increases gallstone formation risk
- Acute kidney injury — Primarily secondary to dehydration from vomiting and diarrhoea
- Hypoglycaemia — More likely when semaglutide is combined with other glucose-lowering medications, particularly sulfonylureas or insulin
- Allergic reactions — Discontinue and seek medical attention for swelling, difficulty breathing, or severe rash
Drug Interactions — What Pharmacists Check Before Dispensing
Semaglutide’s mechanism of slowing gastric emptying creates a pharmacokinetic interaction with any oral medication whose absorption depends on gastric transit time. This is a clinically important point that is frequently underexplained to patients.
- Oral contraceptives — Delayed gastric emptying may reduce absorption of oral contraceptive pills, particularly during the first few weeks of semaglutide initiation. A backup contraceptive method is advisable during this adjustment period.
- Levothyroxine (thyroid medication) — Absorption of levothyroxine can be affected by changes in gastric transit time. TSH levels should be monitored more closely when initiating semaglutide in patients on thyroid replacement therapy.
- Warfarin and other anticoagulants — Changes in dietary intake and absorption kinetics during semaglutide treatment may affect INR stability. More frequent INR monitoring is warranted.
- Insulin and sulfonylureas — Combination use significantly increases hypoglycaemia risk. Dose reductions of insulin or sulfonylureas may be required when initiating semaglutide in patients with type 2 diabetes.
- Oral medications with narrow therapeutic windows — Any medication where small changes in absorption affect efficacy or safety requires closer monitoring when semaglutide is added to the regimen.
What to Do If Semaglutide Is Not Working
If you are not losing weight on semaglutide, consider the following before assuming the medication is ineffective:
- Check your titration timeline — Significant weight loss typically becomes apparent from weeks 8–12 onward, not in the first four weeks. The initial phase is adaptation, not weight loss.
- Review your eating window — Semaglutide reduces appetite but does not prevent overeating during hunger windows. Caloric intake still matters. If nausea has passed and appetite has returned strongly, a dietitian review is useful.
- Check concurrent medications — Several medications directly counteract weight loss: corticosteroids, certain antidepressants (mirtazapine, paroxetine), antipsychotics, beta-blockers, and insulin. A pharmacist or physician should review your full regimen.
- Rule out thyroid or hormonal causes — Undertreated hypothyroidism, PCOS, or insulin resistance can significantly blunt semaglutide response. Lab workup is warranted if weight plateau occurs early.
- Confirm injection technique — Injecting into a lipohypertrophic site (hardened tissue from repeated injections in the same location) significantly reduces absorption. Proper site rotation is essential.
Frequently Asked Questions
How long does it take to see weight loss results with semaglutide?
Most patients begin to notice reduced appetite within the first 2–4 weeks, but meaningful body weight changes typically become visible between weeks 8 and 16. The landmark STEP 1 trial ran for 68 weeks, reflecting that semaglutide is a long-term treatment programme, not a rapid intervention.
What happens when you stop semaglutide?
The STEP 1 trial extension found that patients who discontinued semaglutide after 68 weeks regained approximately two-thirds of their lost weight within 12 months. This confirms that weight regain after stopping is expected — not a sign of treatment failure. Semaglutide manages obesity as a chronic condition; its benefits persist only with continued use, similar to how antihypertensive medication only controls blood pressure while it is being taken.
Is semaglutide safe long-term?
The STEP 5 trial followed patients for two years and found no new safety signals beyond those identified in shorter trials. Gastrointestinal side effects remained the most common adverse events. Longer-term data beyond two years continues to emerge from post-marketing surveillance. The SELECT trial, published in 2023, additionally demonstrated that semaglutide reduces the risk of major cardiovascular events in adults with obesity and established cardiovascular disease — suggesting cardiovascular benefit that extends beyond weight loss alone.
Can I take semaglutide if I have a thyroid condition?
Semaglutide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or MEN2. For patients with common thyroid conditions — hypothyroidism, Hashimoto’s thyroiditis, or well-treated papillary thyroid cancer — the evidence does not show a clinically meaningful increased risk. However, thyroid hormone levels should be monitored, particularly as weight loss itself can affect levothyroxine dosing requirements. Discuss your specific thyroid history with your prescribing physician.
Is Ozempic® the same as Wegovy®?
Both contain semaglutide but differ in their approved doses and indications. Ozempic® is approved for type 2 diabetes at doses up to 2 mg weekly and is used off-label for weight loss. Wegovy® is approved specifically for chronic weight management at the higher 2.4 mg maintenance dose. The titration schedules also differ — do not substitute one product’s dosing protocol for the other.
Key Takeaways
- Semaglutide produces clinically significant weight loss — the STEP 1 trial demonstrated a mean 14.9% body weight reduction at 68 weeks with the 2.4 mg dose
- The dose escalation schedule is medically necessary, not optional — rushing it leads to severe GI side effects that cause most treatment discontinuations
- Semaglutide is a long-term medication — weight returns if treatment is stopped, as shown in the STEP 1 extension trial
- It carries real contraindications including a family history of medullary thyroid carcinoma, MEN2, pregnancy, and severe GI disease
- Drug interactions with oral medications are clinically relevant — your full medication list must be reviewed by a pharmacist or physician before starting
- Maximum benefit requires combining semaglutide with a healthy diet and physical activity — it reduces appetite, but it does not replace lifestyle modification
References
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine. 2021;384:989–1002.
https://pubmed.ncbi.nlm.nih.gov/33567185/ - Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2). The Lancet. 2021;397(10278):971–984.
https://pubmed.ncbi.nlm.nih.gov/33667417/ - Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity (STEP 4). JAMA. 2021;325(14):1414–1425.
https://pubmed.ncbi.nlm.nih.gov/33755728/ - Garvey WT, Batterham RL, Bhatta M, et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nature Medicine. 2022;28:2083–2091.
https://pubmed.ncbi.nlm.nih.gov/35668354/ - Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). New England Journal of Medicine. 2023;389:2221–2232.
https://pubmed.ncbi.nlm.nih.gov/37952131/ - Feier CVI, Faur AM, Muntean C, et al. Assessment of Thyroid Carcinogenic Risk and Safety Profile of GLP-1 Receptor Agonist Semaglutide Therapy. International Journal of Molecular Sciences. 2024;25(8):4346.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11050669/ - FDA Prescribing Information — Wegovy® (semaglutide) injection. U.S. Food and Drug Administration. 2021.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215256s000lbl.pdf